CT mental health providers, schools, or school-based health centers can download the CBITS/Bouce Back application or learn more in the CBITS/Bounce Back pamphlet.
June 20, 2019

Schools can play an important role in helping children recover from traumatic stress. Trauma exposure is common among school-aged children; for example, nearly half of all children ages 6 to 9 experience physical assault.1 While many children exposed to potentially traumatic events will recover with the support of caregivers and natural supports alone, others experience ongoing behavioral health challenges including traumatic stress, posttraumatic stress disorder (PTSD) and difficulties developing healthy relationships.2 Exposure to trauma can also have a profound impact on school functioning, with such children being at greater risk for a variety of concerns including discipline referrals, suspensions, absences, grade retention, and lower academic achievement.3
Public Act 13-178, and the resulting Connecticut Behavioral Health Plan for Children (2014), charges schools with taking an active role in addressing young students' behavioral health needs (including trauma), and Public Act 15-232 encourages (but does not require) school districts to provide trauma-informed care trainings to school employees. However, children impacted by trauma exposure may not be properly identified or receive effective trauma-focused services if staff are not trained in trauma, students are not screened for trauma, and if trauma-focused services are not available. Schools must have quality training in order to ensure access to evidence-based interventions that foster socioemotional and academic success for children exposed to trauma. One resource for districts is Bounce Back, a brief, evidence-based group intervention to help children who are exposed to trauma to build skills and resilience and increase socioemotional and academic functioning. Bounce Back can be one important component of a broader school mental health approach that addresses the wide range of student behavioral health needs from prevention to intervention.
In 2014, the Connecticut Department of Children and Families (DCF) recognized the need to provide schools with resources for students exposed to trauma. DCF funded a statewide dissemination of Cognitive Behavioral Intervention for Trauma in Schools (CBITS) and partnered with CHDI to serve as the Coordinating Center. CBITS is a school-based, trauma-focused group intervention designed for children in grades 5 through 12, and is working in Connecticut to improve student outcomes.4, 5 Since 2014, over 1,200 children have participated in CBITS.
In 2017, recognizing the need for even earlier intervention, DCF and CHDI began disseminating Bounce Back, an evidence-based adaptation of CBITS for elementary-aged children,6 to schools to assist younger students experiencing traumatic stress. All training, consultation, and data reporting is funded by DCF and provided by CHDI at no cost to districts, and districts can even earn performance- based sustainability funding for implementing Bounce Back.
Bounce Back includes ten group sessions, one to three parent sessions, and up to three individual child sessions. Bounce Back helps children to understand, cope with, and recover from trauma exposure by building awareness and skills in the following areas:
The goal of Bounce Back is to assist children with recovering from trauma exposure by building personal and social support systems so that they can feel better, think more clearly in school and at home, develop healthy relationships, seek help when needed, and feel capable of being successful students and adults.
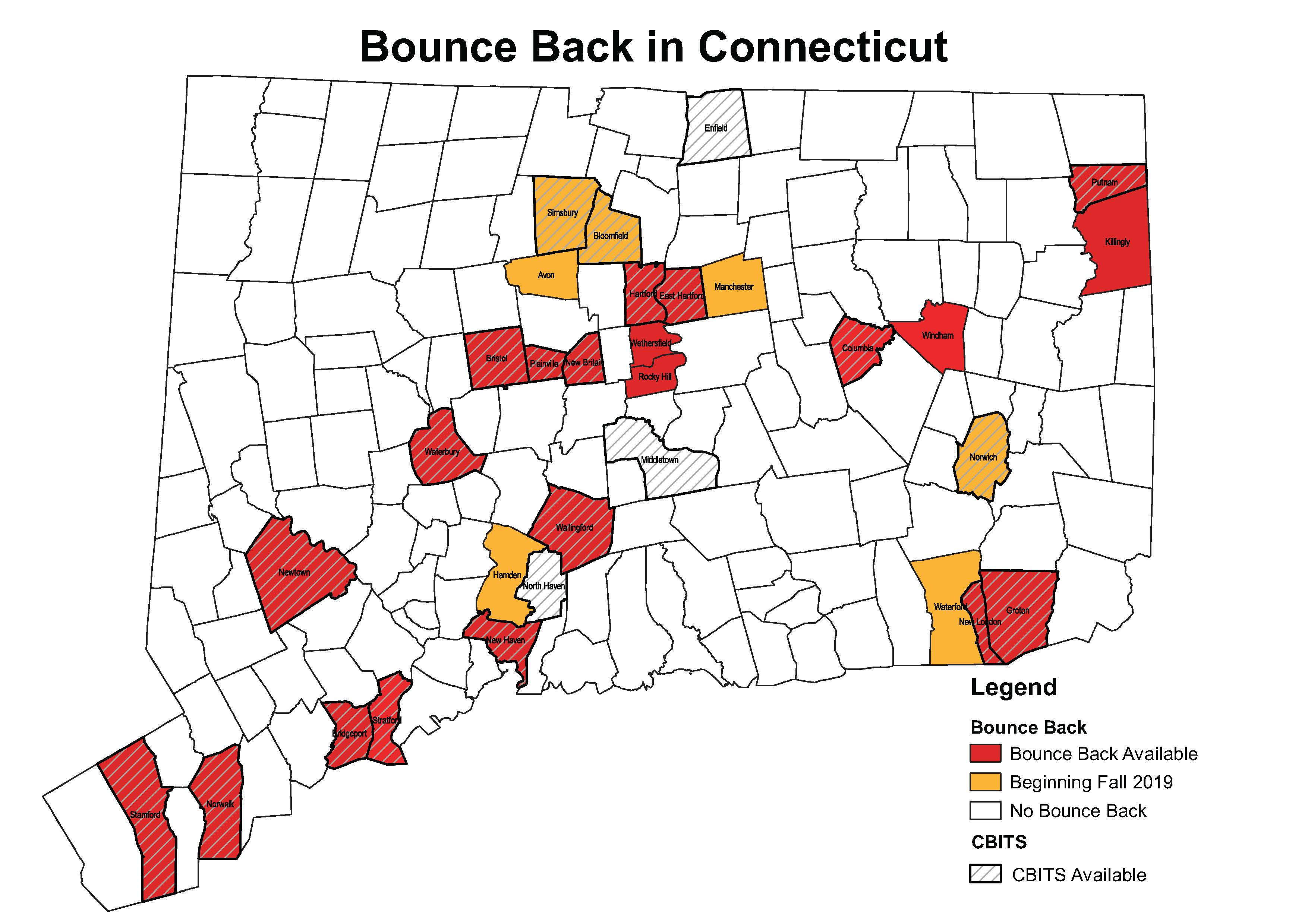
BounceBack is now available at 39 schools in 14 Connecticut districts, and trained clinicians have provided groups to 384 students.
Schools implementing Bounce Back screen their students for trauma to determine eligibility for the groups. More than half (58%) of all students screened qualify for Bounce Back. These children have reported trauma exposure and significant levels of traumatic stress, indicating a high level of need for both identifying and serving students exposed to trauma.
 There is a 93% completion rate among children who begin Bounce Back, a rate that is significantly higher than traditional community-based outpatient care. Approximately 40-60% of children and families drop out of mental health treatment prematurely due to obstacles such as transportation, inconvenient times, and stigma.7, 8 These barriers to care disproportionately affect families from diverse racial, ethnic and economic backgrounds, whereas making treatment available in school settings can mitigate these disparities in service access.
There is a 93% completion rate among children who begin Bounce Back, a rate that is significantly higher than traditional community-based outpatient care. Approximately 40-60% of children and families drop out of mental health treatment prematurely due to obstacles such as transportation, inconvenient times, and stigma.7, 8 These barriers to care disproportionately affect families from diverse racial, ethnic and economic backgrounds, whereas making treatment available in school settings can mitigate these disparities in service access.
 Children receiving Bounce Back show a 75% reduction in symptoms of PTSD following participation in the intervention. In addition, more than half (57%) of children who had a likely diagnosis of PTSD based on initial screening no longer met criteria for a likely PTSD diagnosis after the group, indicating meaningful improvement in traumatic stress that is likely to result in improved health and academic functioning.
Children receiving Bounce Back show a 75% reduction in symptoms of PTSD following participation in the intervention. In addition, more than half (57%) of children who had a likely diagnosis of PTSD based on initial screening no longer met criteria for a likely PTSD diagnosis after the group, indicating meaningful improvement in traumatic stress that is likely to result in improved health and academic functioning.
Results of Bounce Back in Connecticut demonstrate improvement in student outcomes. Caregivers also report high levels of satisfaction with the treatment their child received. With over 600 public elementary schools across the state, many of which may benefit from Bounce Back, Connecticut is still in the early stages of rollout. The following recommendations for school administrators and state policymakers will expand access to Bounce Back for students experiencing trauma.
This Issue Brief was prepared by Diana Perry, Ashley Nelson, and Jason Lang. For more information on CBITS and Bounce Back including how to apply for free training, contact Diana Perry at dperry@uchc.edu or visit https://www.chdi.org/cbits.
REFERENCES
Join CHDI's Email List to get our latest publications and updates on children's health and mental health issues.

