Download a fact sheet on the Early Childhood Trauma Coalition

April 16, 2018

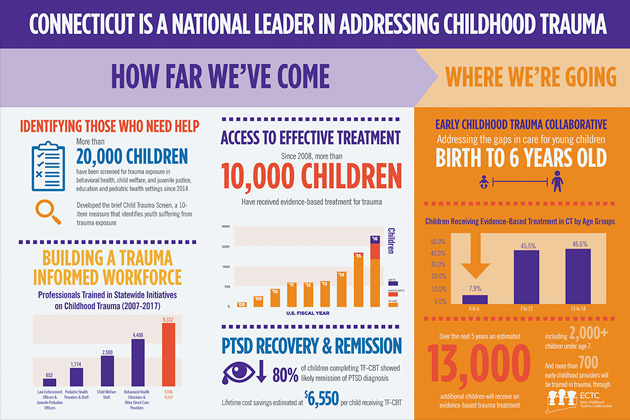
Young children (under age 7) are exposed at high rates to potentially traumatic events such as abuse, violence, and loss of a loved one. Over half of all victims of child abuse in the U.S. are under age six.1 Despite this, young children who are victims of trauma receive trauma-focused behavioral health treatments at much lower rates than older children. Since 2008, of the more than 10,000 children in Connecticut that have received effective trauma treatments, only 800 of these children were under age seven. This treatment gap is concerning, because the rapidly developing brains of young children are especially sensitive to the damaging and lasting effects of trauma exposure.2 Intervening early with children who have experienced trauma reduces the potential for developing posttraumatic stress disorder (PTSD) and other serious behavioral health problems later in life.3 Furthermore, early investment in children’s mental health ultimately pays off many times over in future cost savings.4 This evidence suggests that there is a critical need to better identify young children exposed to trauma, and to build specialized treatment capacity to address their needs.
ARC Supports Parents in Helping Young Children Recover from Trauma
Through a five year SAMHSA grant awarded to CHDI as part of the National Child Traumatic Stress Network (NCTSN), the Early Childhood Trauma Collaborative (ECTC) is helping to address this gap by training clinicians to use Attachment, Self-Regulation and Competency (ARC),5 an effective treatment for young children who have experienced trauma and their caregivers.
ARC is a behavioral health treatment that supports parents (or other caregivers) to help their children address problems resulting from trauma exposure. ARC accomplishes this by helping parents develop the skills they need to assist their children with addressing the negative effects trauma may have on interacting with others (attachment), managing emotions (self-regulation), and meeting developmental milestones (competency). Involving parents in treatment is important because parents of young children have frequently experienced the same traumatic events as their children (e.g. domestic violence, community violence). ARC can help caregivers develop their own skills and simultaneously assist their children with reducing the negative effects of trauma exposure.
Through ECTC, CHDI is training clinicians to deliver ARC primarily to children from birth through age 7 who have experienced trauma. ARC is now available in 11 outpatient behavioral health clinics across Connecticut, and 63 clinicians have been trained to deliver the model. Since October 2017, 150 children under age 7 and their caregivers have received ARC. Preliminary outcomes show a reduction in PTSD symptoms and a large reduction in parents’ own depression symptoms. In addition to ARC, the ECTC initiative is also training providers in three other evidence-based practices: Child Parent Psychotherapy, TARGET, and Child and Family Traumatic Stress Intervention.
Connecticut is Making Progress, However Barriers Remain for Addressing Trauma in Young Children
Increasing the State’s capacity to treat traumatic stress in young children is an important first step in closing the treatment gap. Despite this progress, additional steps are needed to identify and connect families to these effective treatments and ensure policies support the delivery of these treatments for young children and their families.
The current reimbursement rules limit the ability of behavioral health providers to get paid for treating young children. Commercial insurance companies and Medicaid typically require the diagnosis of a mental illness to receive reimbursement; however, formal diagnostic criteria are often not applicable to very young children. As a result, many providers choose not to treat younger children, particularly those under three years old, thus limiting access to early and effective trauma-specific treatment.
Other factors that limit access to trauma-specific services for young children include misconceptions about the impact of trauma on young children, limited awareness and understanding about the behavioral health needs of young children. Raising awareness among preschool teachers, day care providers, home visitors, and others working with young children about the impact of trauma and available services is critical to identifying children who can benefit from treatment and connecting their families to trained providers. Since October, over 400 early childhood staff have received training about trauma in young children through ECTC, and CHDI is currently partnering with the Office of Early Childhood, United Way, and Eastern Connecticut State University to develop sustainable and scalable trauma training curricula for early childhood staff. Improving knowledge about child trauma will ensure that all early childhood providers can effectively identify, support, and refer young children experiencing traumatic stress.
Recommendations to improve services for young children experiencing trauma include:
Provide introductory training in child trauma and available services to all staff in the early childhood workforce.
Revise reimbursement policies for behavioral health services to include trauma-related early intervention services in the absence of a DSM- 5 diagnosis. Adopting the DC: 0-5 criteria for diagnosing young children has been used by other states.
Implement universal screening for traumatic stress in early childhood settings in conjunction with developmental and behavioral health screening and referral mechanisms for effective treatments.
Increase the capacity of the provider network to deliver ARC and other interventions for young children and their caregivers.
REFERENCES
1. U.S. Department of Health & Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. (2018). Child Maltreatment 2016. Available from https://www.acf.hhs. gov/cb/research-data-technology/statistics- research/child-maltreatment.
2. Shonkoff, J. P & Phillips, D. A., (2000). From Neurons to Neighborhoods: The Science of Early Childhood Development. National Academies Press.
3. DeYoung, A. C., Kenardy, J. A., & Cobham, V. E. (2011). Trauma in early childhood: A neglected population. Clinical Child and Family Psychology Review, September 2011(14), 231-251. doi:10.1007/s10567-011-0094-3
4. Heckman, J. J. (2006). Skill formation and the economics of investing in disadvantaged children. Science, 312(5782), 1900-1902.
5. Blaustein, M. E. and Kinniburgh, K. M. (2010). Treating Traumatic Stress in Children and Adolescents: How to Foster Resilience through Attachment, Self-Regulation, and Competency. NY: Guilford Press.
This Issue Brief was prepared by Kim Campbell and Jason Lang. For more information contact Kim at kcampbell@uchc.edu or (860) 679-2907 or visit www.chdi.org/ectc.
Join CHDI's Email List to get our latest publications and updates on children's health and mental health issues.